
My Departure from the World of Consulting – But Not Going Too Far

After 20 years in consulting, I’m excited to share that I’m returning to where my career truly began, working directly with a major local healthcare system right here in my hometown of Boston. Coming back to the city feels both familiar and energizing, and I’m grateful for the opportunity to make a difference my own backyard and honestly….not have to go to the airport!
I want to express my sincere appreciation to the healthcare IT consulting industry and the many leaders, colleagues, and clients who have shaped my path over the years. Your guidance, partnership, and trust have been instrumental in my growth, and I’m deeply thankful for the experiences we’ve shared.
At my core, my passion has always been working with and for hospitals by supporting consultant teams on various client initiatives. Empowering operational teams while helping the client by ultimately improving the end user experience has been such a great experience. This next chapter brings me closer to that mission, and I’m looking forward to contributing more directly across broader platforms for multiple hospital and ambulatory facilities.
I also want to acknowledge something foundational: none of this journey would have been possible without Epic and its EHR platform. Epic has been the backbone of my career, opening doors, shaping my expertise, and connecting me with incredible organizations and people across the country. I’m grateful for the impact it has had on my professional life.
And while I’m stepping out of consulting, my consultant blog isn’t going anywhere. I’ll continue writing about the ongoing changes shaping our industry, from the evolution of healthcare IT and EHR strategy to the rapid rise of AI and automation. I’ll also keep sharing insights on career development for both consultants and full‑time professionals navigating this fast‑moving space. My goal remains the same: to help others grow, adapt, and thrive in a field that never stops changing.
Here’s to the next chapter — grounded in purpose, shaped by experience, and focused on the communities we serve, with plenty more to explore and write about along the way.
ChatGPT for Healthcare: What It Means for Consultants in our EHR World

The introduction of ChatGPT for Healthcare marks yet another shift in how technology will support clinicians, analysts, and operational teams. Woke up to multiple articles and announcements today on this and dug right in to understand what this is and how it might impact workflows and operations. I also wanted to compare the capability with what Epic and Oracle are introducing. Thought I would share some of those findings and a couple of thoughts.
Firstly, unlike the consumer version of ChatGPT, this healthcare version is built with the privacy, security, and data‑handling expectations required in clinical environments. It’s designed to connect securely to medical records and other health data sources, allowing it to generate summaries, draft documentation, and support clinical reasoning. For those of us who have spent years helping organizations navigate EHR workflows, this represents a new layer of intelligence that sits above the system rather than within.
What makes ChatGPT for Healthcare different is its structure that runs on GPT‑5 models that have undergone physician-led testing and are designed to operate within HIPAA aligned environments. It separates health data from general ChatGPT interactions, uses enhanced encryption, and provides the kind of guardrails that health systems expect. In other words, it’s not a consumer chatbot repurposed for healthcare but rather a clinical tool that can safely interact with sensitive information while supporting the EHR workflows clinicians already know.
Where this gets interesting for us consultants is how it fits into existing EHR ecosystems. Epic and Oracle are already building their own AI assistants and ambient documentation tools, and those capabilities will continue to grow. But ChatGPT for Healthcare doesn’t compete with the EHR, it complements it. Both Epic and Oracle will always own the structured, workflow‑embedded intelligence inside the EHR. ChatGPT for Healthcare becomes the flexible layer around it: summarizing chart data before a visit, drafting patient instructions, helping analysts write SQL or reporting logic, generating prior authorization narratives, or supporting training and policy development. It’s the kind of tool that can reduce administrative burden without replacing the EHR as the system of record.
From a consultant’s perspective, this is where the opportunity lies. Every time a new technology like this enters the market, it expands the skill set required to support hospitals and health systems. I feel like this is a message I write about in almost every post as of late. As consultants, we need to understand how to integrate these tools and how to align them with governance and compliance structures, as well as look at redesigning workflows so clinicians can benefit without adding risk or complexity.
Would love to hear from anyone implementing this. Notice the list of hospitals already planning to install in the original press release.
Read the Announcement Here – Introducing OpenAI for Healthcare | OpenAI
Epic Optimization Is Evolving: More on Client Led Innovation

Hospitals continue to prove that some of the most meaningful innovations don’t come from vendors; they come from the people closest to patient care. I came across a great article and example this morning that talked about University Hospitals’ recent work inside Epic to proactively identify patients at risk for axial spondyloarthritis, an underdiagnosed inflammatory condition. Their approach, highlighted in the Becker’s article, shows how clinical teams and IT can use Epic not just as an EHR, but as a true engine for early detection and better outcomes.
As someone who has spent two decades in consulting, these stories always hit me in a particular way. They remind me that every time a hospital builds something like this, a screening tool, a new way of surfacing risk…it expands what’s possible inside Epic and raises the bar for the rest of the industry. It also pushes consultants to keep learning, adapting, and staying ahead of the curve so we can support organizations as they design, refine, and operationalize these new capabilities. I think of the workflow impacts, application dependencies, and overall change management approach.
This is the kind of innovation that strengthens the value of an Epic investment while creating new opportunities for advisory work, workflow redesign, and clinical adoption support. And it’s a reminder that the future of healthcare IT will be shaped not just by software releases, but by the creativity of the hospitals and those consultants who know how to turn technology into better care.
Check out the Becker’s Article – Why University Hospitals built an Epic application to detect arthritis – Becker’s Hospital Review | Healthcare News & Analysis
Altaris Buys Tegria: A Familiar Story in Our Industry

2026 is off to a big start with news in the Healthcare IT world. Tegria’s sale to Altaris is an interesting headline for sure. I had to do some reading to understand Altaris’s positioning in the market, and now I think I get why this is worth talking about. Thought I would share some thoughts.
With Altaris now backing Tegria as a fully independent company, the firm is stepping into a much more ambitious role in the healthcare IT market. They’ll no longer be tied to Providence’s internal priorities as Tegria now has the capital, freedom, and strategic mandate to scale nationally, expand its service lines, and compete directly with firms like Nordic, Chartis, Accenture, and Optum. Well, I list Nordic but remember, Nordic was acquired by Bon Secours just a few years ago. Interestingly doing the exact opposite of Tegria. I think this shift creates a very different landscape and certainly creates variances in priorities of their mission to the healthcare community.
For independent consultants and even small boutique firms, there could be an opportunity. Tegria’s growth strategy will likely include acquiring niche capabilities, expanding its subcontractor network, and partnering with specialists who can help it win larger transformation and outsourcing deals. This is exactly what we did when we sold the EHR division of Nuance. As the company broadens its footprint across EHR optimization, revenue cycle modernization, cloud migration, and digital transformation, it will need talent and expertise with external consultants and/or small companies who are uniquely positioned to provide support.
Their top areas of focus, based on what I’ve read, include:
• EHR implementation and optimization
• Revenue cycle technology services
• Digital transformation support
• IT outsourcing and managed services
• Analytics and interoperability solutions
I always scratched my head when Providence Health bought all these consultant firms and created Tegria in the first place. Seemed like a conflict of interest. But now they are no longer just another regional IT services group. It has an opportunity to become a bigger national player with private equity momentum behind it. Consultants and small companies who understand where Tegria is headed, and can align their offerings with its expanding portfolio, will find themselves well positioned for potential partnerships or contracts. This will be fun to watch and I wish them luck. Does anyone have thoughts or ideas, maybe who have worked with Tegria? Leave comments below…
Here is the Press Release – Altaris Acquires Tegria | Altaris, LLC
2026 Airline Fee Policies: What’s Real and What’s Marketing
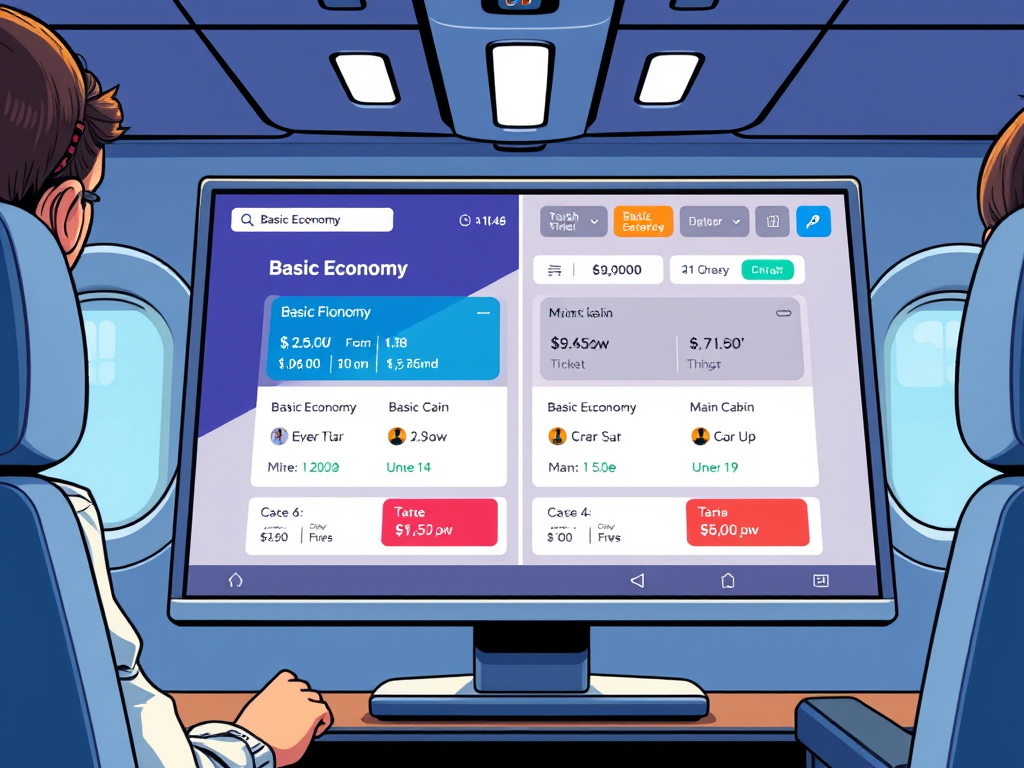
Many of us have not been flying as much due to hybrid or remote contracts. Its been over 6 months for me and this week while looking at flights, I found myself scratching my head on how the website was showing flight costs that were not what I am used to seeing. The little red X marks had me concerned about changes in cancellation fees and upgrade eligibility. After some digging, I knew some of us would have stories of being tricked.
All major U.S. airlines have had a policy in regards to no change or cancellation fees for standard economy tickets since Covid. Delta was one of the first to make this permanent, eliminating fees for Main Cabin and premium fares on flights originating in the U.S. American and United followed with nearly identical policies, and today all three allow free changes on most tickets. Southwest, for those who love this airline, has never charged change fees for any fare class.
But the real story sits beneath the surface. While Main Cabin flexibility has become the norm, Basic Economy remains a highly restricted product across all major airlines. Delta, American, and United all block changes and cancellations for these fares, and low‑cost carriers like Frontier and Spirit still charge fees that the big airlines have abandoned. This creates a two‑tiered experience: a flexible “consumer‑friendly” Main Cabin and a rigid, no‑changes‑allowed Basic Economy designed to look cheap but feel costly once the restrictions become clear.
That’s why airline websites almost always display Basic Economy as the default lowest fare. It’s not a glitch…it’s a revenue strategy. By leading with the cheapest number, airlines anchor the customer on price, then reveal the limitations only after you click on the lowest fare. Consumer advocates have criticized this as confusing or even “bait‑and‑switch,” especially in cases like American Airlines, which has been called out for making fare transparency harder to navigate. And while each airline handles the presentation differently, the pattern is consistent: Basic Economy is intentionally positioned to drive upsells to Main Cabin, where the no‑change‑fee promise actually applies.
In other words, the industry has embraced flexibility, but only for the fares they want you to buy. The headline policies sound generous, and in many ways they are, but the digital storefronts still steer travelers toward the most restrictive product first. Understanding that dynamic is the key to understanding modern airline pricing: the flexibility revolution is real, but the marketing strategy hasn’t changed at all
Most of you know I am a Delta loyalist, so I did some reading just to spell this out, and not favor Delta over other airlines…well, as best as I could. The bottom line that we all need to be aware of is it is deceptive across all airlines.
The pattern is industry wide, though some airlines are more aggressive than others.
- Delta, American, and United all prominently display Basic Economy as the lowest fare, even though it does not allow changes or cancellations.
- The restrictions are often only visible after clicking into the fare details.
- Analysts and consumer advocates have repeatedly criticized this practice as confusing, opaque, and intentionally designed to push upsells.
- Southwest is the only major U.S. airline that avoids this issue entirely because it does not offer Basic Economy.
Has anyone find themselves fooled and stuck with a ticket they can’t cancel or get upgraded? Share in the comments below.
Hospitals Are Becoming Tech Companies — Impact for IT Consultants

In a meeting I had just a couple of weeks ago with a Chief Innovation Officer of a healthcare system, I learned of their internal development of a new AI solution. It made me wonder who else might be doing this, and after just a few articles, I found there was a big trend in AI and overall technology development happening internally, vs hospitals going out to buy the solution needed. I wanted to share just a few examples here and my thoughts on potential impact to consultants.
Organizations including Mass General Brigham, Mayo Clinic, Cleveland Clinic, and Stanford Medicine are all building platforms inside their clinical environments, validating them on real patient data, and then exploring commercialization pathways, whether through spinouts, licensing, or joint ventures. These new tools are proving valuable enough that they can scale beyond their home hospital. The common theme I found appears to be that newly internally developed technology is being treated as strategic intellectual property, not just an internal tool.
These systems also share a similar pattern where they build a solution that solves deeply operational problems. In reading multiple articles, the focus appears to be on workflow automation, unstructured‑note extraction, population health risk stratification, and care‑pathway optimization. Before any commercialization step, the tools are deployed internally at scale, stress‑tested across multiple specialties, and integrated into clinical workflows before turning it into a company with a product.
For those of us in Healthcare IT consulting, this shift is going to reshape the landscape in a pretty fundamental way. As more health systems start building and commercializing their own products, we won’t just be advising on technology adoption; we’ll be helping organizations evaluate, integrate, and even compete with tools that originate inside other hospitals. It changes the mentality of just supporting Epic or Oracle because the clients we support may now be both buyers and creators in the AI/technical marketplace.
Hospitals spinning out tech companies will expect consultants who understand not just EHR integration, but IP strategy, go‑to‑market planning, interoperability standards, and the operational realities of scaling technology safely. In other words, the consulting value proposition shifts from implementing tools to helping health systems become technology-driven organizations, or in this case, even an AI/technology vendor.
Regardless of your area of focus as a consultant, we’ll all need to adjust to a broader capability of support. All these changes imply that hospitals are becoming product creators, not just adopters. I just wrote about continued learning as my new year’s resolution, so hearing about all these hospitals taking on development of their own technologies only reinforces the need to keep up on all these great new tools being developed. 2026 is going to be an interesting year in Healthcare IT!
Anyone working with a client that this is a priority? Please feel free to share in the comments area below.
Here is the Mass General Brigham Press Release – Mass General Brigham Announces New AI Company to Accelerate Clinical Trial Screening and Patient Recruitment | Mass General Brigham
New Year, New Edge: How to Stay Competitive in our Industry

I’ve been contemplating my commitment for 2026 and thought I should have a resolution to ensure continued professional growth. I recently read that one powerful direction for New Year’s resolutions is to treat your own professional development as a structured, ongoing practice, rather than a reactive one. That might look like committing to a quarterly skills audit, identifying what the next stage of your skill sets and/or leadership level requires. A commitment to watch where the industry is shifting, and which capabilities will matter most, as AI continues to reshape operations. I’ve been pretty good at doing this, but I think I’ll take it to the next level this year.
My first thought is to add one new competency each quarter, whether it’s learning about an emerging AI operations tool with Epic and/or other software, or refining leadership systems that scale with a startup’s growth. I continue to be involved with start-ups whose software is exceptional, but needs strategy and leadership to take it to market and grow. I’m thinking this might help me at the executive level to keep one step ahead of the curve. If you are a consultant, I love the idea of a quarterly skill set exercise, sort of like what Epic used to do with NVTs.
On the financial side, I also want to focus on strengthening long‑term stability while still giving room to pursue various opportunities. Another great recent article I read was on creating a “financial strategy review,” which basically treats your own compensation and wealth planning with the same rigor you would bring to a company’s operating model. That could include optimizing cash flow, setting clear savings or investment targets, or building a framework for evaluating equity opportunities in startups so you can confidently balance risk and upside.
Finally, I am really an advocate for continuous learning, so I am definitely going to round out this year’s resolutions with a commitment to ongoing self‑education, perhaps dedicating a set number of hours each month to exploring new IT and AI advancements. As my career plans for this year will be something new and away from staffing, I’m also thinking of experimenting with tools hands‑on, or attending IT/AI specific workshops to keep me plugged into what’s next.
Check out these great articles for some ideas:
https://www.salary.com/resources/hr-glossary/master-comp-planning-stay-ahead-with-smart-strategies
Love to hear what you all are focusing on for the new year. Leave your comments below.
A $50 Billion Shift: How Rural Health Funding Might Redefine IT Support Needs
The press release from the US Department of Health and Human Services is big news for IT consultants. The newly announced $50 billion Rural Health Transformation Program represents one of the largest federal investments ever made in rural healthcare, with every state receiving substantial funding beginning in 2026. The initiative aims to expand access to care, strengthen the rural workforce, and modernize facilities across all 50 states. For rural hospitals, this signals a major shift toward more technology for care delivery, particularly in preventive services, behavioral health, emergency care coordination, and chronic disease management. All of which will require stronger digital infrastructure and more sophisticated technical support than many rural facilities currently have. Funding like this helped so many of us get contracts and work during Meaningful Use, so I can’t help but wonder if this also could open more doors for future opportunities.
A significant portion of the funding is dedicated to modernizing rural health infrastructure, including upgrades to equipment, cybersecurity, interoperability, telehealth, remote patient monitoring, and digital workflow tools such as AI scribing, which we are all used to via Nuance or Epic. These investments will dramatically increase the volume and complexity of IT systems rural hospitals must deploy, maintain, and secure. States will need to roll out new models, regional data sharing platforms, and clinically integrated networks. Additionally, rural hospitals will need more robust networking, 24/7 system monitoring, and specialized support for interoperability across disparate EHRs and care settings.
The program also encourages innovative care models and value‑based payment structures, which depend heavily on accurate data capture, analytics, and reporting. This will push rural hospitals, many of which currently operate with minimal IT staffing, to adopt more advanced data systems and require ongoing technical assistance, training, and cybersecurity oversight. This could be great news for so many of us in the consulting world!
In short, the federal investment will expand care access and modernize rural health delivery, but it will also create a surge in demand for IT support, managed services, cybersecurity expertise, and long‑term digital transformation planning across rural healthcare organizations. Feel free to leave comments. Curious what folks think about this news.
See the full Press Release here – US Department of Health and Human Services
Not another AI article…just a quick realization check

Our entire industry of Healthcare IT is racing to sprinkle “AI” on everything in sight. Much like hard to fill consulting staffing needs, this is the tech world’s version of finding a unicorn. But in reality, a lot of what’s being marketed as artificial intelligence, in the various EHR systems today, might just be closer to automation vs sentient software.
Epic has embraced the AI label across its platform, from clinician assistants to patient-facing tools. At their 2025 Users Group Meeting, the company highlighted hundreds of new AI features, and at HIMSS demos, some 60+ new products, including Emmie, ART, and Penny, that were all aimed at helping clinicians with charting, documentation, and administrative tasks.
The reality? Most of these capabilities resemble what many refer to context aware automation, including:
- drafting prior authorization responses based on structured data
- suggesting codes after a visit
- summarizing chart sections for easier workflows.
These are truly just workflow automation, not the much hyped AI future of technology releases that we read about every day. These are all still ultimately guided by human decisions and rely on existing clinical processes, not independent clinical judgment.
Check out this great Epic article on CNBC.
Since Oracle acquired Cerner, the messaging has leaned heavily into new AI driven capabilities. The new Oracle Health EHR platform is described as “AI-driven intelligence” built into workflows, able to surface insights, handle voice-activated commands, and trim documentation burden.
This fall the press releases and news articles were endless, including this fun read Oracle Ushers in New Era of AI-Driven Electronic Health Records
But a closer look shows most of this is still just automation, including:
- converting speech to text and structuring notes,
- pulling up relevant chart data on keyword requests,
- auto-suggesting orders or navigation clicks.
These are valuable productivity enhancements, which everyone can benefit from, but they don’t think or diagnose on their own. They automate repetitive tasks that clinicians used to do manually.
There are genuinely some AI-centric tools that I’ve seen, including systems that analyze medical images, flag deterioration risk patterns, or predict clinical outcomes based on massive datasets. Check out Nuance/Microsoft, which partners with both Epic and Oracle. But let’s all be clear and recognize that most EHR-embedded features today are task automation with AI branding that tout age old promises of reducing clicks (ever hear that one before?), creates draft texts (been around for years), and directly improves workflows.
Thoughts on how “AI” is driving your optimization project support efforts? Share your comments here.
Double Dipping in Consulting: Where the Line Gets Crossed

There was a recent post on LinkedIn that received hundreds of hits and dozens of responses regarding double dipping. It got me thinking about the scenarios where it could be normal to be working for more than one client…but also, I’ve known many that may have been pushing the line. So let’s dive into this subject, and please feel free to share your thoughts on this.
In the world of EHR consulting, the term “double dipping” carries ethical, contractual, and professional implications. At its core, double dipping refers to a consultant working two or more paid engagements at the same time, without disclosure to the client(s), while presenting themselves as fully committed to each role. While working multiple jobs isn’t automatically illegal, double dipping crosses into unethical territory when deception, overlapping hours, or conflicts of interest are involved. The original post on LinkedIn focuses on the idea that consultants who are double dipping are stealing, lying, and cheating their clients. Ok, let’s dissect this some more.
Double dipping typically occurs when a consultant accepts multiple high-commitment projects simultaneously and bills each client as if they were working exclusively for them. This can include billing the same hours to two clients, logging into multiple Epic instances or other environments during overlapping work periods, or hiding one engagement from another. These behaviors raise red flags for consulting firms and health systems alike and can expose consultants to allegations of fraud, breach of contract, or termination.
Here are some rather common forms of double dipping:
- Simultaneous Epic Projects: Taking on two full-time, or near–full-time, Epic contracts at once during demanding phases like implementations, optimizations, or go-lives.
- Conflict of Interest: Supporting competing health systems or vendors, which can risk exposure of sensitive workflows, build strategies, or proprietary information.
- Fraudulent Billing: Charging two clients for the same block of time could escalate into billing fraud.
- Deception and Non-Disclosure: Intentionally hiding another role from an employer or client, violating trust and contractual obligations.
- Epic System Monitoring: Epic environments can detect concurrent logins across different client systems, which may trigger internal audits or investigations. See many of my past articles on being black listed.
Double dipping is not really applicable when supporting efforts through managed services and/or call center roles. For example, a consultant may be assigned scheduled support hours for one organization while simultaneously providing managed services coverage for another. Because these roles often involve “availability-based” billing rather than strict project milestones, clients expect their agents to be only partially assigned to them. There are situations where the client wants call agents to be 100% assigned to their organization, and in those examples, double dipping would not be appropriate.
Not all secondary work is unethical. Moonlighting can be acceptable when roles are low commitment, schedules do not overlap, and all parties are informed and consenting. For example, a consultant might take on limited advisory work or short-term troubleshooting outside of core hours. We can’t assume malicious behavior when all clients are aware, and the consultant is 100% transparent.
Consulting relies heavily on trust, transparency, and professionalism. While the flexibility of consulting can create opportunities for additional work, crossing the line into double dipping introduces significant ethical and legal risks. Whether in project-based consulting, managed services, or call center support, disclosure and honesty are essential. When in doubt, clear communication and written approval are the only safe paths forward. I believe that there is a competitive nature that also warranted many of the comments on the LinkedIn post. I would love to hear your thoughts. Share your insights on the subject in the comment section.
Click on my image below for my Professional Profile


Comments